
 Tribune Group GmbH Inc.
Tribune Group GmbH Inc.
Nationally Approved PACE Program
Provider for FAGD/MAGD credit.
Approval does not imply acceptance by
any regulatory authority or AGD endorsement.
7/1/2024 - 6/30/2028.
Provider ID# 355051
Tooth Apexification Using Bioceramic Materials
Sponsor: Angelus
Author: Maria Antonieta Veloso Carvalho de Oliveira
Co-author: Nayara Rodrigues Nascimento Oliveira, Jessica Monteiro Mendes, Thallys Rodrigues Félix, Luís Henrique Araújo Raposo, Paulo Vinícius Soares
RESUME
A 12-year-old female patient came to the Dental Hospital of the Federal University of Uberlândia (HO/UFU) reporting a spontaneous, diffuse, intermittent, long-lasting pain exacerbated by chewing plus cold and hot stimuli. Tooth 35 had a coronary access performed in a private dental practice six months earlier. Radiographically, unsatisfactory coronary access, thickening of the periodontal ligament, a diffuse periapical lesion and the presence of an open apex were observed (Figure 1A).
During the first appointment, the provisional material was removed, and the coronary access was refined with an inactive tip multilaminated bur (Endo Z, Angelus) (Figure 1B). This was followed by instrumentation of the cervical and middle thirds, after a calcium hydroxide associated with saline solution was used as intracanal dressing.
After one month, the patient returned for an intracanal dressing change and a little change was observed in the appearance of the periapical lesion. It was then decided to use a bioceramic intracanal dressing (BIO C TEMP, Angelus) (Figure 2A). Two intracanal dressing changes were performed, with a two-month interval between them (Figure 2B). During the removal of the intracanal dressing in the second change, it was possible to feel the formation of mineralized tissue in the apical region and regression of the periapical lesion.
Four months after the beginning of the treatment and 30 days after the last intracanal medication change, the root canal was filled. The bioceramic medication was removed. After the final irrigation and drying of the canal, a plug was made with bioceramic repair cement (BIO-C REPAIR – Angelus) (Figure 3).
With the apical seal well positioned, the root canal filling was performed using the technique of vertical and lateral condensation. The bioceramic root canal sealer (BIO-C SEALER, Angelus) in combination with gutta percha cones was inserted into the root canal with its own tip, positioned 3.0 mm short of the plug (Figure 4).
The patient did not report any painful symptoms during the months of treatment. In the follow-up session, six months after root canal filling, the tooth did not show sensitivity to the percussion tests. Radiographically, there was regression of the periapical lesion and tissue formation in the apical region of the tooth (Figure 5).
IMAGES

Figure 1A. Radiographic aspects after removal of the provisional restoration.
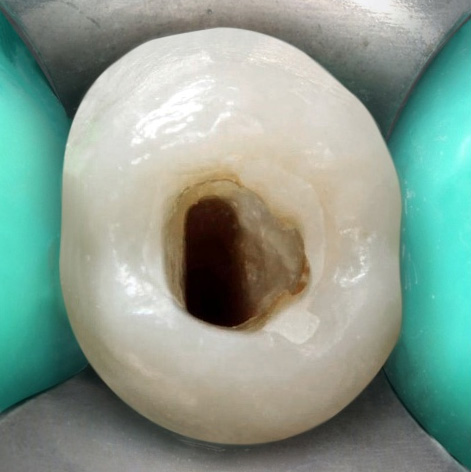
Figure 1B. Clinical aspects after refinement of the coronary access.

Figure 2A. Bioceramic intracanal medication.

Figure 2B. Radiographic aspect inside the root canal after the first change.

Figure 2C. Radiographic aspect inside the root canal after the second change.

Figure 3A. Bioceramic repair cement.
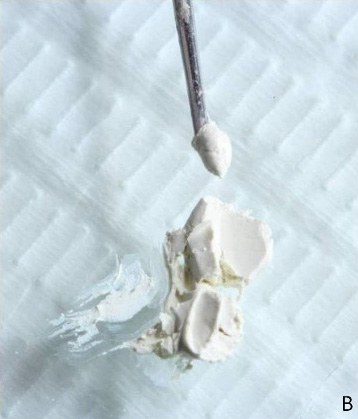
Figure 3B. Aspect of the material.

Figure 3C. Insertion of the material in the root canal.

Figure 4A. Bioceramic root canal sealer.

Figure 4B. Placement of the sealer.
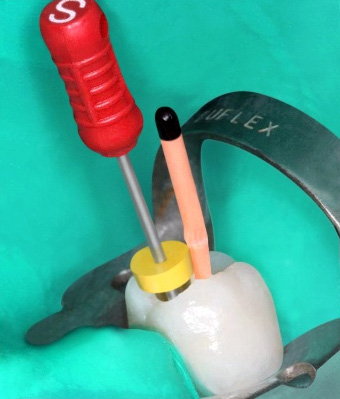
Figure 4C. Insertion of gutta-percha cones into the root canal.
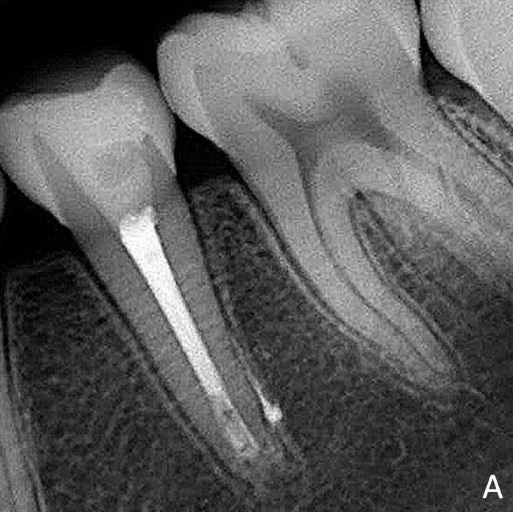
Figure 5A. Radiographic aspect after filling.

Figure 5B. Radiographic aspect after six months of follow-up.