
 Tribune Group GmbH Inc.
Tribune Group GmbH Inc.
Nationally Approved PACE Program
Provider for FAGD/MAGD credit.
Approval does not imply acceptance by
any regulatory authority or AGD endorsement.
7/1/2024 - 6/30/2028.
Provider ID# 355051
Endodontic retreatment with root perforation using MTA repair cement and MTA based sealer
Sponsor: Angelus
Author: Nayara Rodrigues Nascimento Oliveira Tavares
Co-author: Jéssica Monteiro Mendes, Alexia da Mata Galvão, Maria Antonieta Veloso Carvalho de Oliveira
RESUME
A 42-year-old female patient came to the private practice complaining of spontaneous pain on tooth number 36. According to the patient file, endodontic retreatment had been performed on it. During the clinical exam, the tooth presented positive vertical and horizontal percussion tests. Radiographically it showed a lesion in the furcation region, and endodontic treatment (Figure 1).
The restoration was removed using a round and conical safe tip bur (Endo Z, Angelus). It was possible to verify the presence of whitish material in the mesial root (Figure 2A). The material was removed, and the perforation was visualized in the distal portion of the mesial root, close to the canal entrance (Figure 2B).
In the same session, the filling material was removed (Figure 3A) with Retreatment files in the distal canal and Hedstroen manual files in the mesial canal, due to suspected fracture of the file in the apical third. The fractured file was confirmed (Figure 3B) with a radiograph. A Calcium hydroxide intracanal dressing was placed during two sessions.
After removing the medication with 2.5% sodium hypochlorite, the gutta-percha cone was tested and kept inside the canal as a form of protection to seal the perforation (Figure 4) with MTA-based repair cement (MTA HP Repair, Angelus).
After verifying the adaptation of the repair cement (Figure 5 and 6), the canals were filled with an MTA based endodontic sealer (MTA Fillapex, Angelus) and gutta-percha cones, using the lateral condensation technique (Figure 7 and 8).
The tooth was provisionally restored. A radiograph was taken (Figure 9A). A post, buildup, and crown restoration were planned for a later session. Twelve months after the completion of treatment, the patient returned for control with no spontaneous pain, and no radiographic changes (Figure 9B).
IMAGES

Figure 1: Initial x-ray.
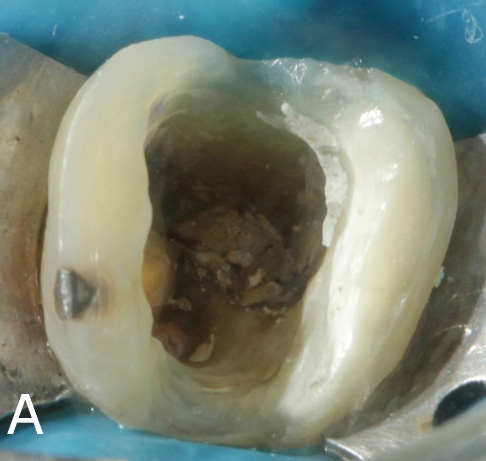
Figure 2: A. Whitish material in the mesial root.

Figure 2: B. Presence of root canal perforation.
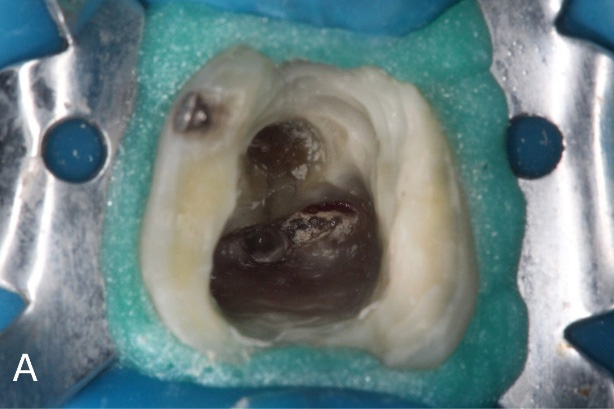
Figure 3: A. Removal of filling material
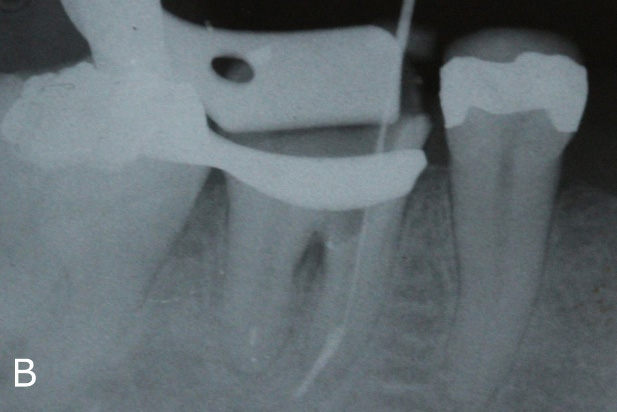
Figure 3: B. X-ray to confirm the presence of a separated file.
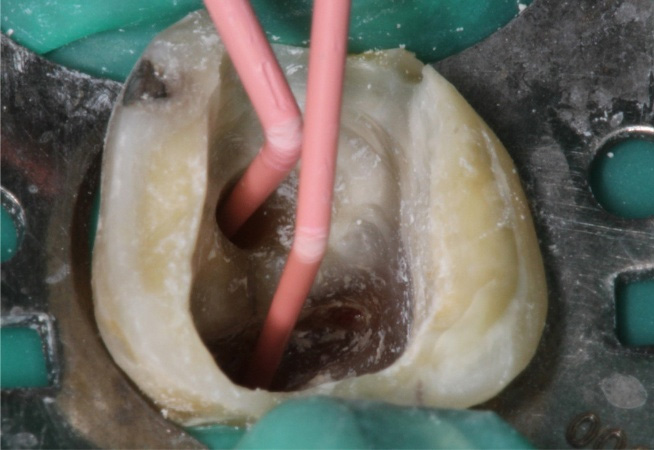
Figure 4: Gutta-percha cones protecting the entrance of the root canals.
Figure 5: MTA HP Repair manipulation.

Figure 5: MTA HP Repair manipulation.
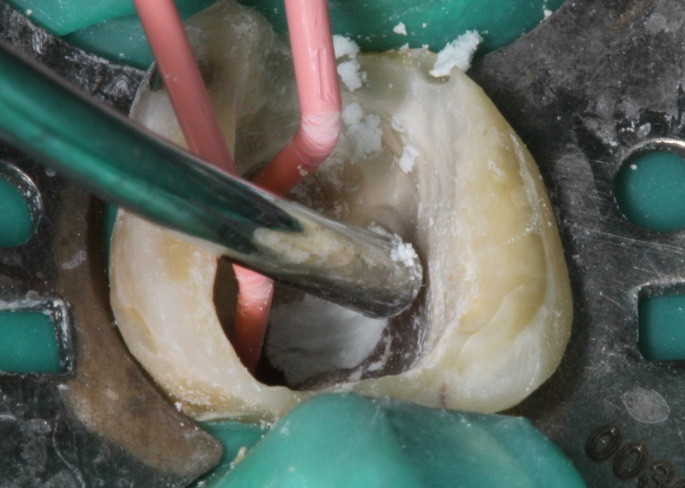
Figure 6: Insertion of cement in the root canal perforation.

Figure 7: MTA based endodontic sealer – MTA-Fillapex.

Figure 7: MTA based endodontic sealer – MTA-Fillapex.
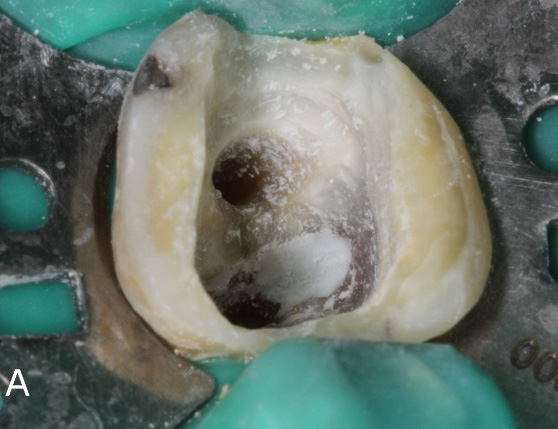
Figure 8: Clinical aspect after sealing the perforation (A).

Figure 8: Clinical aspect after filling the canals (B).

Figure 9: A. Final radiography.
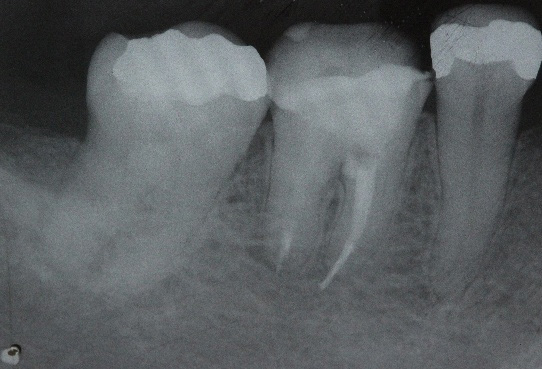
Figure 9: B. Follow-up after Twelve months.